- The paper introduces mmHRR, a contactless system using mmWave radar to monitor heart rate recovery post-exercise with high precision.
- It employs a three-stage pipeline combining adaptive VMD‐based heartbeat extraction with composite sliding window peak detection.
- Experimental results on 14 subjects show a 3.31 bpm error, outperforming previous methods by 71% while ensuring robustness under varied conditions.
Introduction
Heart rate recovery (HRR) immediately post-exercise is a clinically significant measure of cardiac autonomic function and is predictive of mortality risk in patients with cardiovascular disease. Traditional HRR monitoring relies on either medical-grade or wearable contact sensors, both of which suffer from cost, comfort, and user experience limitations. Existing contactless methods using wireless signals (WiFi, UWB, acoustics) are typically designed for low-noise conditions with subjects at rest and do not effectively capture the rapid, non-stationary, and entangled physiological signals observed immediately after exercise.
The work "mmHRR: Monitoring Heart Rate Recovery with Millimeter Wave Radar" (2503.22202) introduces mmHRR, a contactless system for accurate HRR estimation using COTS mmWave radar. It addresses fundamental technical difficulties: rapidly-varying heart rate, interference from respiratory harmonics, and low signal-to-noise ratio due to body and limb motion after exercise. The mmHRR framework features a specialized signal processing pipeline integrating adaptive target tracking, robust vibration extraction, and HR estimation via composite sliding windows.
Signal Characteristics and Challenges
The mmHRR system confronts two intersecting challenges in post-exercise monitoring: rapid HR changes (up to 32 bpm decrease in 60 seconds) and severe harmonic interference from non-sinusoidal respiration. These create transient, non-stationary signals where respiratory harmonics often overlap with cardiac frequency bands, confounding traditional frequency-domain analysis.
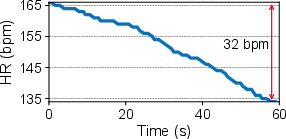
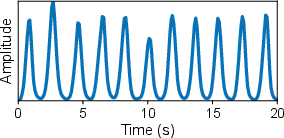
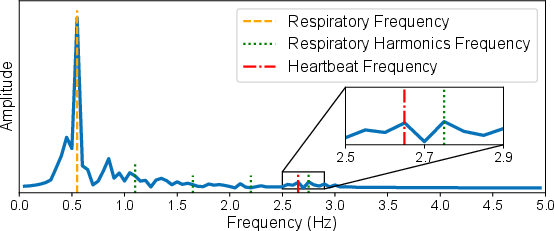
Figure 2: Non-stationary heartbeat signals and overlapping respiration harmonics structure the post-exercise estimation challenge.
System Architecture
mmHRR’s three-stage processing pipeline consists of Signal Preprocessing, Heartbeat Signal Extraction, and Heart Rate Estimation.

Figure 1: Overall architecture comprising radar acquisition, dynamic tracking, adaptive signal decomposition, and robust HR estimation.
- Signal Preprocessing: The proprietary pipeline leverages FMCW-based phase trace extraction, continuity correction for range bin jumps, and cascaded temporal filtering (0.2–3.4 Hz). Signal differencing amplifies the relative contribution of heartbeat and harmonics for improved subsequent decomposition.
- Heartbeat Signal Extraction: The chest motion signal—composed of respiration, multiple harmonics, heartbeat, and noise—is decomposed with an improved variational mode decomposition (VMD) algorithm. The authors introduce correlation (via Pearson coefficient) and energy loss coefficient criteria for bandwidth parameter autoselection, ensuring effective mode separation while avoiding noise-dominated or aliased components.
Mode selection utilizes an analysis of frequency relationships: respiratory harmonics are explicitly identified, and the remaining component with distinct frequency or maximal overlap (in the event of coincidence) is assigned to the heartbeat.
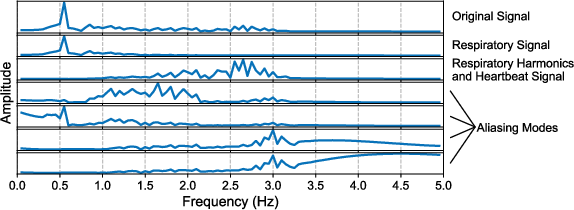
Figure 3: Example decomposition during mode aliasing due to poor parameter selection—illustrates the need for new criteria.

Figure 4: VMD successfully separates heartbeat and harmonics—the foundation for robust HRR estimation.
- Heart Rate Estimation: The extracted heartbeat mode is smoothed and amplitude-normalized. Peak detection employs a composite sliding window, dynamically adjusted to recent HR estimates, allowing fine-grained temporal localization despite rapid rate changes. This approach supersedes traditional spectral analysis, which lacks requisite temporal adaptability and suffers under short time windows.
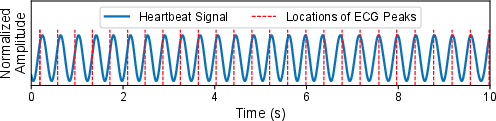
Figure 5: Synchronized peaks between the processed mmWave signal and ECG ground truth confirm high-fidelity extraction.
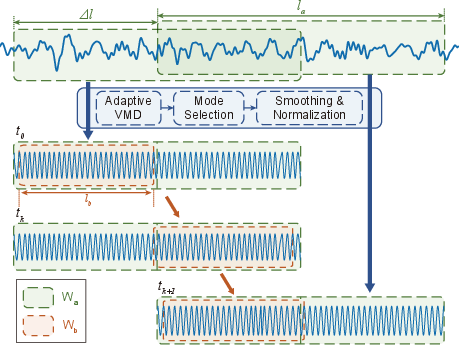
Figure 6: Depiction of the composite sliding window algorithm integrating adaptive segmentation with robust peak counting.
Experimental Validation
Implementation was on a TI IWR1642BOOST radar platform, with experiments involving 14 subjects in a classroom environment. The evaluation benchmarked mmHRR against mmHRV—a SOTA mmWave-based cardiac monitoring system optimized for resting subjects.
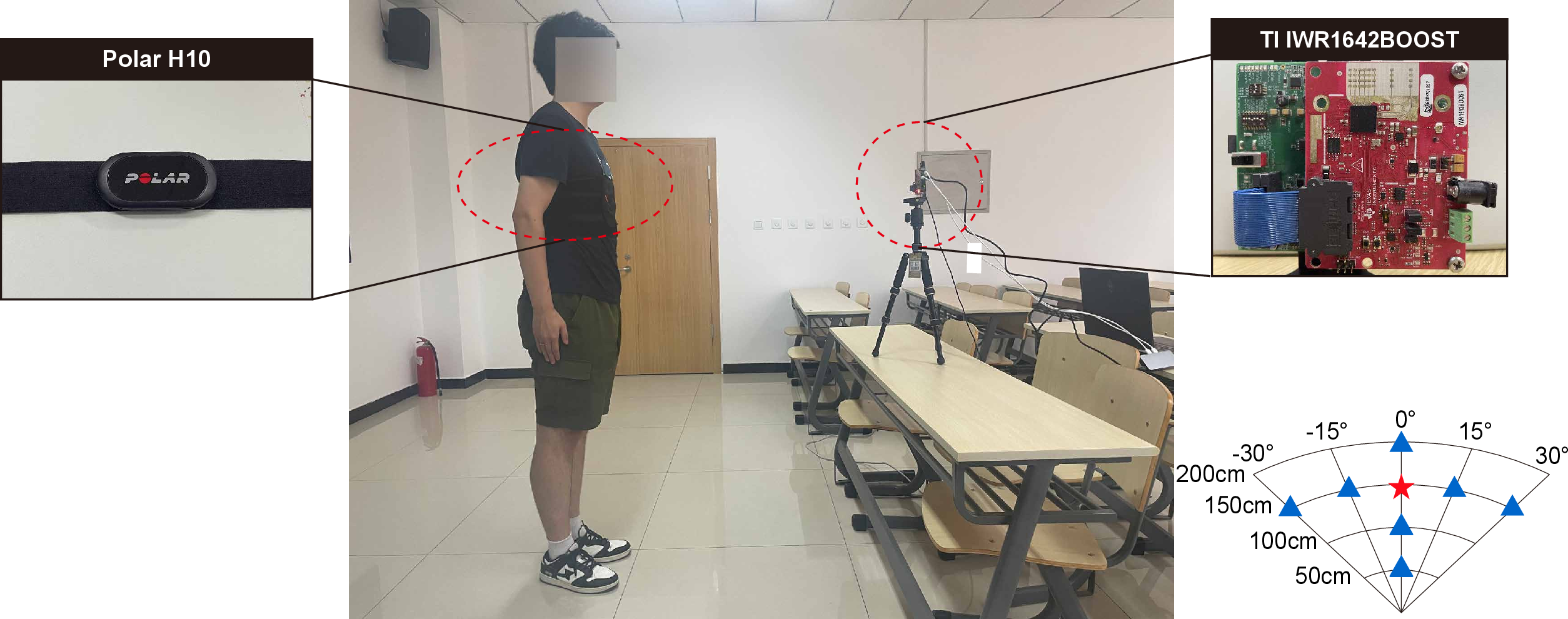
Figure 7: Laboratory deployment configuration demonstrating mmHRR hardware and user arrangement.
Key Results
- Accuracy: mmHRR achieves an average HR estimation error of 3.31 bpm—71% lower than SOTA mmHRV.
- Stability Across Conditions: Performance is minimally affected by initial (post-exercise) HR, user-sensor distance up to 2 meters, target angle, or user heterogeneity.
- Robustness: Maintains high accuracy under different postures (seated, moving), simultaneous monitoring of multiple users, and across episodes where HR remains stable or transiently rises post-exercise.
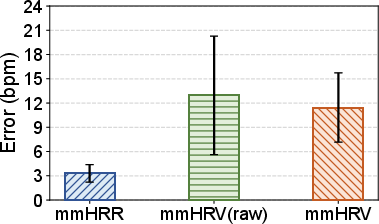
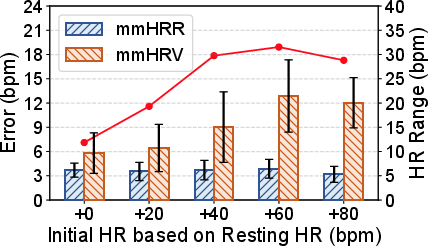
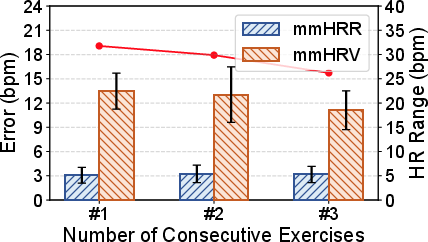
Figure 8: mmHRR consistently outperforms mmHRV baseline in overall error distribution.
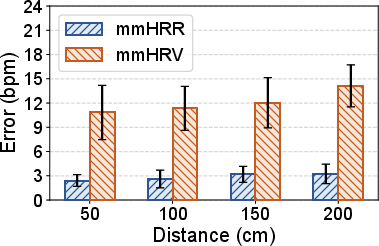
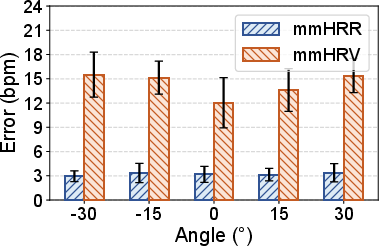
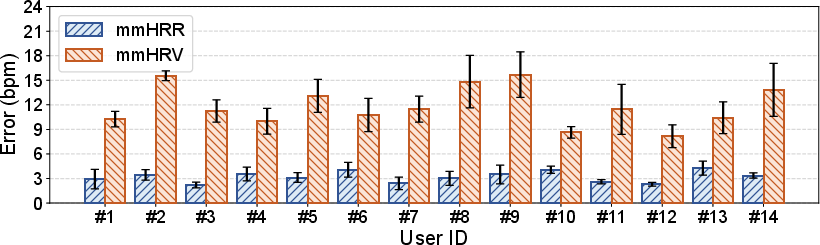
Figure 9: mmHRR accuracy is robust to user–radar distance variations, maintaining low average error.
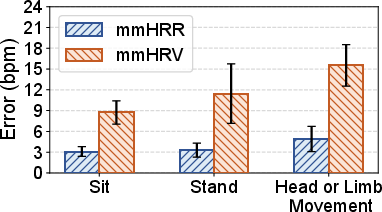
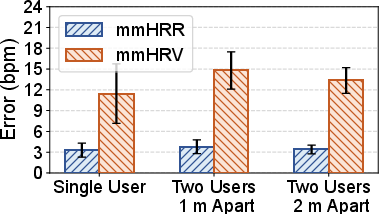
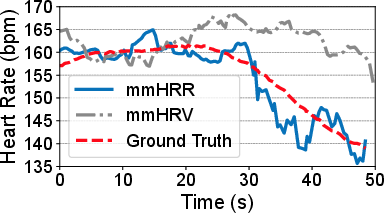
Figure 10: The system handles postural transitions and mild movement with minor increases in error.
Contradictory Claims and Strong Results
- The paper demonstrates that existing frequency-domain and naive VMD approaches (such as mmHRV) systematically fail for post-exercise scenarios, contradicting claims of SOTA accuracy from prior work which assumes stable/resting HR.
- Only through application-specific adaptation (composite sliding windows, adaptive VMD) can robust HRR estimation be achieved.
Implications and Future Directions
Practical Impact
mmHRR's contactless architecture, low error margin, and robustness across environmental and physiological variables make it suitable for real-world deployment in clinical, home, and athletic settings. It extends the operational domain of radar-based physiological monitoring from passive, resting users to the essential post-exercise recovery window.
Theoretical Implications
- The study establishes that adaptive, multimodal signal decomposition—guided by context- and artifact-aware parameterization—can overcome fundamental limits of stationary spectral analysis in biosignal sensing.
- This approach may generalize to other non-stationary physiological signals (e.g., stress detection, arrhythmia detection in ambulatory settings).
Future Research
Potential research directions include expansion to multi-person, multi-radar scenarios; embedding online learning for subject-specific calibration; utilization of neural signal processing architectures to further suppress non-cardiac motion artifacts; and extension toward unsupervised event detection in unstructured activity.
Conclusion
mmHRR represents a technically rigorous contactless solution for heart rate recovery monitoring, setting a new performance baseline through adaptive signal processing specific to non-stationary, post-exercise biosignals. The methodology and empirical results challenge prior assumptions regarding mmWave cardiac sensing and open opportunities for further AI-driven advancement in contactless health monitoring.